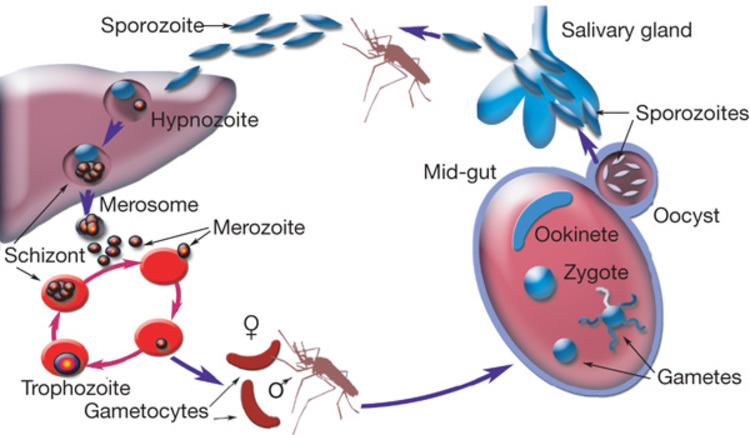
A simple malaria cycle
Julia Mugadzaweta Features Writer
Zimbabwe has recorded a huge milestone in the fight against malaria, but lately fresh threats to the impressive record have emerged.
The incessant rains and consequent flooding have created breeding conditions for mosquitoes, a prospect likely to raise malaria cases.
Government, however, believes they are in control of the situation.
Considering the challenges that have rocked Zimbabwe’s health sector in recent times, can the situation be contained?
Officials are of the opinion there should not be panic in the wake of a possible outbreak given Zimbabwe’s track record.
Dr Joseph Mberikunashe, the programme manager of the Malaria Control Unit in the Ministry of Health and Child Care, said the rains have posed a challenge but the situation is under control.
“The recent flooding has, of course, derailed our progress. However, it hasn’t made much of an impact as we have made great improvements towards the treatment of malaria,” he said.
Dr Mberikunashe said intervention programmes had already begun.
“We have teams that were moving around during the pre-malaria season doing door to door residual spraying.
“There was also distribution of treated mosquito nets and our institutions in potential risk areas have received enough medical equipment enabling them to treat patients should a problem arise,” he said.
However, a fresh scare has already been reported in Bikita and Beitbridge districts.
The Herald recently reported that five people in Beitbridge had died from malaria since the beginning of the rainy season and about 800 people tested positive.
Dr Mberikunashe said they had already contained the situation.
“Those suspected of having malaria cases were treated and those who sought medical attention quickly got immediate responses.
“The number of people we treat seasonally has not risen despite the reported cases,” he said. “In Malipati, rivers were flooded, this caused delays in delivering treatment.”
He said clinics across the country had enough stocks of malaria treatment drugs.
Cross-border movement is also a malaria transmitter especially in areas like Beitbridge.
“Beitbridge is affected because it’s a transit town therefore people access medical attention after the effect, not necessarily that they have contracted it in that area,” Dr Mberikunashe said.
The Ministry of Health and Child Care considers cross-border malaria a priority area for investigation so evidence-based decisions can be made to decrease the malaria burden, which is highest in three provinces bordering Mozambique.
Health and Child Care Minister David Parirenyatwa admitted the effects of cross-border transmissions.
“The cross-border movements complicate the situation and most of the cases are imported or those people in transit,” he said.
Matabeleland South has in the past recorded high malaria cases with Beitbridge being the highest followed by Gwanda.
Plumtree had a few cases, but Government intervention in Matabeleland South contained the situation.
Matabeleland South is the only province that has advanced to the pre-elimination stage of malaria treatment.
Zimbabwe Hospital Doctors’ Association president Dr Edgar Munatsi said the rains received this season increased chances of malaria cases.
“We have been receiving heavy rains which have probably resulted in stagnant waters that are a breeding ground for malaria infested mosquitoes and it is a one contributing factor,” he said.
Dr Munetsi encouraged people in malaria-prone areas to be cautious and always seek treatment when travelling.
“Usually we encourage pregnant women not to travel to malarias areas but if the need arises, we encourage them to take malaria drugs,” he said.
Preventative measures, he added, should always be observed.
“Pregnant women and children under five, who live in high transmission areas, should always sleep under a treated mosquito net, wear long sleeved cloths and seek treatment immediately if they suspect any case of malaria contraction.”
He, however, lamented infrastructure damage by the incessant rains.
“The provision of medical services has been greatly affected by the destroyed infrastructure which has made health facilities inaccessible and even the flooding itself prevented access to medical attention,” he said.
According to the Malaria Operational Plan document 2017, discussions are underway between the Zimbabwe National Malaria Control Programme and Mozambican National Malaria Control Programme.
In Zimbabwe, malaria accounts for between 30 to 50 percent of outpatient attendances in the moderate to high transmission districts, especially during the peak transmission period.
Transmission is generally seasonal, starting from around November to the end of May, with the peak period being between March and May.
However, a Zimbabwe National Statistics Agency (Zimstat) report revealed that over 50 percent of the country’s population is at risk of contracting malaria despite the introduction of several measures to combat the disease.
The most vulnerable group which is prone to malaria transmission are children under 5 and pregnant women.
Control of malaria in pregnancy (MIP) was adopted as a policy in Zimbabwe in 2004 to be implemented in the moderate to high-burden malaria transmission areas, with 30 districts designated for MIP interventions.
Improvement in malaria in pregnancy indicators showed that in 2013 almost 61 percent of pregnant women received treatment to prevent malaria.
In 2014 Health Management Information System (HMIS) data indicates 66 percent of pregnant women in the targeted areas received the same preventative treatment.
However, it remains a major challenge in some provinces, districts, and wards.
The malaria incidence rate in 2014 stood at 39 malaria cases per 1 000 population but went down to 25 malaria cases per 1 000 population in 2015. Malaria incidence rate refers to the number of new cases of malaria per 100 000 people each year.
Malaria incidences declined by 79 percent from 136 per 1 000 people in 2000 to 29 per 1 000 people in 2015, surpassing the Millennium Development Goals set target of 75 percent decline.
Mortality declined by 57 percent from 1 069 deaths in 2003 to 462 deaths in 2015.
According to Zimbabwe District Health Information System 2 (DHIS2) data, approximately 83 percent of all malaria cases and 50 percent of all malaria deaths in 2014 originated from three eastern rural provinces: Manicaland, Mashonaland East and Mashonaland Central.
Forty-two percent of all cases and 26 percent of all deaths were recorded in Manicaland.
Seasonal and geographic variations in malaria transmission have shown close correspondence with the country’s rainfall pattern.
In general, the major of malaria transmission areas receive the highest rainfalls.
Data shows that the country has also surpassed the global 2015 Roll Back Malaria Partnership target for countries to have reduced malaria incidence by 75 percent by December 2015.
According to the National Malaria Control Programme’s latest figures, incidence declined by 86 percent from 2004 to 2012.
However, from 2012 to 2013, incidence rose 32 percent from 22 to 29 deaths per 1000.
In year 2015 the rate increased again to 40 /1 000, a 38 percent change from 2013.
Most positive cases occurred in districts or areas of high-moderate seasonal malaria transmission.
Malaria symptoms are headaches, body fever and flu-like symptoms such as muscle ache, fatigue and vomiting. Despite the interventions and progress made, mosquitoes are said to have grown resistant to commonly used repellants.
- Feedback: jmugadzaweta@gmail.com